Cover Up?
We felt that we were not getting the truth from a very early stage. Even in the very first RCA meeting we had on March 14th 2018, which was recorded, when we suggested things were not transparent, the chair of the meeting Annie Oakley who was the Corporate Governance manager said QUOTE “I can absolutely tell you that this has not been covered up I promise you that.”.
Once you have read the facts below, you can make up your own mind, what is your conclusion?
This from the Kirkup report into East Kent Hospitals Maternity services - He is Referring directly to Harry's case
1.112 This pattern of behaviour by the Trust, clearly evident in this case, recurred in many others that we examined. It included denying that anything had gone amiss, minimising adverse features, finding reasons to treat deaths and other catastrophic outcomes as expected, and omitting key details in accounts given to families as well as to official bodies. Although we did not find evidence that there was a conscious conspiracy, the effect of these behaviours was to cover up the truth.
1.113 Even had none of the previous failings been known – and they were – baby Harry’s death should surely have been a catalyst for immediate change. In fact, it required public remonstration by a coroner over two years later, precipitated by the persistence, diligence and courage of baby Harry’s family, to reveal an organisation that did not accept its own failings, considered itself above scrutiny or accountability, and consistently rejected the opportunity to learn when things went wrong.
The following facts are why we firmly believe there are serious questions to be answered.
Root Cause Analysis (RCA) Meeting - In our recorded, three and a half hour Root Cause Analysis meeting the Trust told us unequivocally that the locum Registrar's CV had been signed off by a consultant before he started work. Only after we pushed for answers, did it later transpire that he had not been signed off at all. This means that the Trust's 4 month long investigation had seemingly failed to identify that the locum had been working without any checks or sign off whatsoever. The very fact that there was no sign off by email as claimed, led us to believe that there was no such system otherwise it would have been flagged. At inquest the Medical Director told the court that they had been "unable to identify who had employed the locum". This, we see as wholly implausible.
In addition, we later discovered that this had been the first locum job Dr Spyroulis had ever taken. Again, nothing in the RCA and no duty of candour statement from the Trust to show that they had discovered this. We suspect that they hadn't discovered it until long after they published their RCA report.
Refusal to refer Harry's death to the coroner - We asked on numerous occasions and were told unequivocally that there was no need to inform the coroner as the cause of death, Hypoxic Ischemic Encephalopathy (HIE) was known. We have this in writing and on tape and it was repeated in the RCA report, signed off at board level by Dr Paul Stephens and Dr Sally Smith. In the recorded RCA meeting of March 14th 2018, Annie Oakley the meeting chair who was not a clinical member of staff, on questioning, admitted that Harry's death was "preventable" and that the care was "inadequate". Therefore, it can only be concluded that sometime before the date of our meeting, these facts were known by senior consultants/managers/directors and yet they still refused to call the coroner.
Our contention that Harry's brain damage was caused 7 days earlier by their actions was ignored. Internally, the Trust from a very early stage on their internal reporting stated that Harry's condition and death were an "unexpected outcome" see the document HERE and look at the top right hand side "Poor Neonatal outcome - Unexpected" and on the left "E - Death - Incident directly resulted in the death of the person(s) affected". This is unequivocal proof that the Trust knew their failings had caused Harry's death, yet they still refused to contact the coroner even when specifically asked to do so by the family on multiple occasions.
By late August 2018, in a meeting with Dr Paul Stevens, Medical Director, the Senior Coroner for Kent told the Trust that Harry's case should have been notified earlier and that from that date ALL baby deaths must be reported by this Trust. It was also noted that the senior coroner said that failure to report Harry's death could be viewed as "obstructing the coroner". By October 2019 our coroner ruled that Harry's inquest was to be an Article 2 inquest, Article 2 of the European Convention on Human Rights, Right to life, the highest form of inquest available. Harry's was not a marginal case in any way shape or form and had to be reported.
You will see from the document here that we notified the coroner on March 15th 2018 at 9.55 in the morning. The Trust had said they would finally refer to the coroner during the meeting we had the previous day (March 14th) however, we had no faith that they would do so. As it happened, we were right, the Trust took a further 5 weeks and 3 days to do so, and only then because we chased the Medical Director twice.
Senior Response - In a letter from the CEO Susan Acott, on January 30th 2019 in response to our complaint She says "........during the RCA meeting, it was reiterated that at the time of Harry's death, given the cause of his death was known, it was felt Harry's case did not require referral to the Coroner. However it was accepted that as you still had concerns a referral to the coroner was undertaken" It later transpired at Harry's inquest in a statement by the Medical Director that in a meeting with the senior coroner for Kent in August 2018, over 5 months BEFORE this letter from the CEO, they were told that Harry's death should have been referred and, that not doing so could be seen as "obstructing the coroner". So why, we ask, in January 2019 was Susan Acott the CEO still saying that the eventual referral was made because we still had concerns rather than because they were duty and morally bound to do so? Please remember that the senior governance officer who chaired the meeting in March 2018 had said that Harry's death was preventable and the care given was inadequate.
We later learnt that baby Archie Powell, born February 10th 2019 at QEQM, died 14th Feb 2019 was not referred to the coroner - BBC article HERE says "The trust, which is at the centre of an independent investigation into maternity care and had failed to inform the coroner of Archie's death at the time" This means that 6 months AFTER the Trust were told to report ALL baby deaths, they still were not doing so. We look at this as clear evidence that outside scrutiny was avoided at all costs. This refusal has led to a significant loss of valuable learning and accountability.
We consider the failure to notify the coroner was a deliberate and gross failing and would constitute a charge of misconduct in public office.
Failure to keep the placenta - The placenta was not kept which was against the Trusts own published guidelines and those of the Royal College of Pathologists. The Root Cause Analysis Investigation (RCA) told us that they only kept placenta when an infection is suspected and in Harry's case it was not. However, in the transfer document from QEQM to WHH it says "Suspected Sepsis". If this wasn't enough, at our March 14th meeting we were told that since Harry's death they had changed policy and that they had purchased pots in which to put placenta and made arrangements with WHH where the pathology would be carried out. Surely this had to mean that before this time, no placenta were kept? Finally, the MBRRACE-UK report filled out by the Trust states that the Placenta was kept and used for histology to determine the cause of death. The coroner’s expert witness said - "In this case examination of the placenta would have been extremely helpful in identifying any other contributing factors to Harry’s condition at birth." and another said "It is my opinion that not retaining the placenta, following a delivery of this nature, fell below the standard expected of any reasonable and responsible body of registered midwives."
Child Death Notification form - This is a mandatory form filled out for all child deaths from 1st breath to 18 years. The Trust filled this form out on November 10th to say that Harry's death was "expected" when of course to us and, as it turned out, the coroner, it was not at all. We challenged this and were told that as life support was to be removed the death was expected 24 hours before. Again, we challenged this and said that it ignored the cause of the brain damage altogether, they still stood by their decision. The ticked "expected" box was accompanied by a benign statement that would attract no attention up the line, you can see the statement here. Harry's own hospital notes from November 3rd said that it was an "unexpected outcome". It wasn't until the last week in August 2019 when we saw the coroners own expert witness report that said "It was not acceptable for the treating team at William Harvey Hospital to conclude that the death was ‘expected’. The death was explained by the presence of severe hypoxic ischaemic brain injury, however the aetiology of the hypoxia ischemia required appropriate consideration and investigation." It would be fascinating to see all Child Death Notification Form's in all baby deaths, how do they compare with what the parents would say? In the coroners conclusion he said that the decision to report Harry's death as "expected" was "incomprehensible".
RCA Investigation - The RCA was carried out by Dr Clare Redfearn the consultant who was the clinical lead in maternity, who was effectively investigating her own team, the consultants and doctors that she worked with and potentially the policies and procedures she had herself instigated. It was her very first RCA. However, she was assisted in the investigation by Dr John Seaton who was head of Women's Health and very experienced. The neonatal side of the investigation was carried out by Dr Kwok Sean Mun the consultant who looked after Harry at WHH, he wrote Harry's death certificate, he arranged the child death notification form, he refused to contact the coroner and he's department filled out the MBRRACE-UK report. They were assisted by Matron Peymaneh Halijou who was on duty on the ward as matron, the morning Harry was born. All of this is totally against NHS England guidelines (here) which states on page 23 that investigations should not be carried out by anyone treating the patient or working with anyone treating the patient, see extract ( blue) at the base of this page from the NHSE document. We raised this on numerous occasions with the Trust but were told it was as independent as it could be and that it was overseen by senior executives. You will also see from the front page HERE that Dr Abigail Price who treated Harry on the day of his birth was also said to be on the investigation team. However, when we challenged this, she asked to have her name removed, saying she was not part of this team?
You will also note the senior executive sign off of the RCA by Dr Rfidah Elhussein (Peadiatric Consultant), Ursula Marsh (head of Midwifery), Dr Paul Stevens Medical Director and Chief Nurse Sally Smith. How, we ask, could all of these people have approved this document?
RCA Inaccuracy -
In the RCA it clearly states in black and white that the locum doctor, Dr Christos Spyroulis, had 2 years’ experience as a registrar. It later became apparent that this doctor had only been a registrar for 9 months. No one at the Trust could identify where their claim of 2 years had come from. We now have a copy of his CV, and he didn't even claim this himself. On examination, the locum doctor's CV showed clearly that the maximum time he could possibly have been a registrar was 1 year. This information is there in black and white if you just work dates back from details given. Are we to believe that no one investigating could read a CV we wondered?
The RCA also states that the resuscitation of Harry was to NLS guidelines, "The descriptions and steps taken were appropriate as per NLS guidelines." it clearly wasn't and this failure was verified by various witnesses at inquest but especially the coroners own expert witness. In the witness box, the expert said that he would have failed every member of the team in resuscitation on even the most basic course that he runs. This proved to us that either the investigation was not carried out properly or they were seemingly covering up what they found. Incompetent or cover-up? There are only 2 choices in our minds.
RCA Independent scrutiny - The RCA was sent off to Maidstone and Tunbridge Wells Trust by way of scrutiny before it was published. This, we were told proved their independence and that they were keen to show us that the RCA had been carried out to the highest standard. However, the external scrutineer was not sent any medical notes or CTG scans so could only look at the report itself but not verify any of it. She made a point of saying that she was surprised that no criticism was levelled at the on-call consultant. A comment regarding the on-call consultant was later rather crassly squeezed in at 1a on the RCA before final publication. Why, we ask, was one of their senior colleagues not singled out for obvious failings before being prompted? We learnt much later that the exact same criticisms of how incidents were investigated and consultants not criticised were levelled by RCOG in their 2015 audit.
The consultant concerned, Anastasia Goumenou, was later made an IP at Harry's inquest due to the damning comments of the coroner’s own witnesses and the evidence against her. The GMC have since said - "Dr Goumenou’s failure to attend when told about the delay in delivery and need for intervention in theatre was seriously below the expected standard, and we agree that Dr Goumenou’s fitness to practise may have been impaired at the time." However, they declined to take any disciplinary action.
RCA family complaint - The RCA clearly states
11/02/2018: The family have submitted a formal letter of complaint. This is being addressed through the Serious Incident investigation process and through the complaints process. However, when we wrote to the CEO in December of 2018 to chase the response to our letter, we were told by her that the complaint had not been treated as a formal complaint................
MBRRACE-UK Report - This is a statutory report that is filled out for all babies or mothers who die or babies that sustain brain damage. It is run by the Nuffield Trust at Oxford University for the government with the express aim of analysing baby death data and in so doing, reducing baby deaths in the UK. At the time of Harry's death, the UK was the 3rd worst in Europe for baby deaths and recently, Jeremy Hunt has said that if the UK could match Sweden in neonatal survival rates, 1,000 babies a year would be saved, that's nearly 3 a day.
We asked to see Harry's report as a Freedom of Information (FOI) request. We were told that this was not a FOI issue as the report was in Harry's clinical records, the request was passed by the FoI team to the clinical records department. This in itself was odd as we already had Harry's notes and it wasn't there? The clinical records department emailed us a very poor copy of a report but it was the Each Baby Counts report for the RCOG. We asked again and were told they didn't have it. By this time, we were in touch with MBRRACE-UK who told us that the hospital did have it and to ask again. We were told "no" yet again. Eventually we got the report from MBRRACE-UK as they advised us to apply to them under a FoI.
When we got it, we found it was full of really important errors or downright lies, depending on your perspective. Such things as the placental histology was used to determine the cause of death was polar opposite to the truth, it hadn't been kept at all. The date of onset of labour and care was said to be November 1st at 00:00 it wasn't, it was over 5 hours earlier. It said that the case had been discussed with the coroner, it hadn't until we did it. Rotational forceps were attempted, they weren't. They said that the Apgar score at 1 minute and 5 minutes was not available, they were in Harry's notes! The final part was the most shocking of all, were there any delivery complications was answered with "None". We wrote to the Medical Director to ask where the information comes from for the MBRRACE report and we were told the patients notes. Clearly in Harry's case they were not, so where did this false information come from we wonder?
In addition, the fact that the MBRRACE-UK report was, by admission of the Trusts own FOI department part of Harry's notes, why was it withheld from the family in clear breach of Duty of Candour?
The coroner ruled that there were a number or important errors in Harry's MBRRACE report and that all MBRRACE reports should be checked for accuracy. As at January 2021 The Trust had not corrected Harry's report. We have to ask ourselves why?
Post-mortem Bloods - When Harry's body was sent to St Thomas' for his post-mortem he was accompanied by a letter to give the details of his birth in order to help the pathologist try to find the cause of death. Harry's cord blood results were sent off but the bloods taken around 45 minutes later in SCBU were not sent at all. The cord bloods showed a hypoxic issue but one that was recoverable, the results of the SCBU bloods however showed that a massive hypoxic insult had taken place between birth and SCBU. What possible reason could there be for these results to be withheld?
Reporting to CCG - Any serious incident has to be reported to the local Clinical Commissioning Group within 72 hours, this is part of the governance contract the Trust has with the NHS. Harry's death was not reported until November 10th the day after he died. We queried this and were told that it wasn't considered a serious incident until he died.....................we found this surprising, hurtful and a real demonstration of the toxic culture that was present at that time. How can a perfectly normal baby receive the severest brain damage where an immediate RCA investigation is raised and yet it was not considered a serious incident until he died? Who was it that was in charge of that decision and why?
RCOG report CEO denial - The full audit of the Trust maternity services was carried out in November 2015 and led to an "extreme" corporate risk register entry in June 2016. Susan Acott CEO started her role in October 2017 but told the BBC's Michael Buchanan in an interview in February 2020 that she had not seen the report until December 2019 and was unaware it had been commissioned. However, in a letter from Susan Acott 10 months before on 31st January 2019 she mentions the RCOG report and the action plan that followed. "CRR26 focussed on reports from the RCOG and LSA............" and "CRR48 incorporates the outstanding actions from the existing action plans (including the RCOG Action Plan)........" How can a CEO be unaware of an "extreme" risk on the boards risk register for over 2 years? How can she deny any knowledge when she wrote about it nearly a year previously? Link to Susan Acott interview HERE
Death Certificates and Reporting - It has emerged during our investigation that the reporting of neonatal deaths needs the utmost scrutiny. Harry's death certificate is 042363 and is a "Medical Certificate of cause of death of a live-born child dying within the first 28 days of life" another child, Child A whose certificate we have seen was filled out 50 weeks before Harry. The sequential numbers show that including Child A and Harry there were 43 neonatal deaths at WHH alone in that 50 week period. The Trust report that there were just 20 such deaths for the entire Trust in this period. Assuming QEQM also have their own book of certificates, they are definitely physical certificates and not digital, how can the figures be even close to true? were there really 43 neonatal deaths at just William Harvey Hospital in that 50 week period? If not, a detailed and audited explanation is needed. (Go to the base of Harry's Legacy page to see the reported neonatal deaths by the Trust)
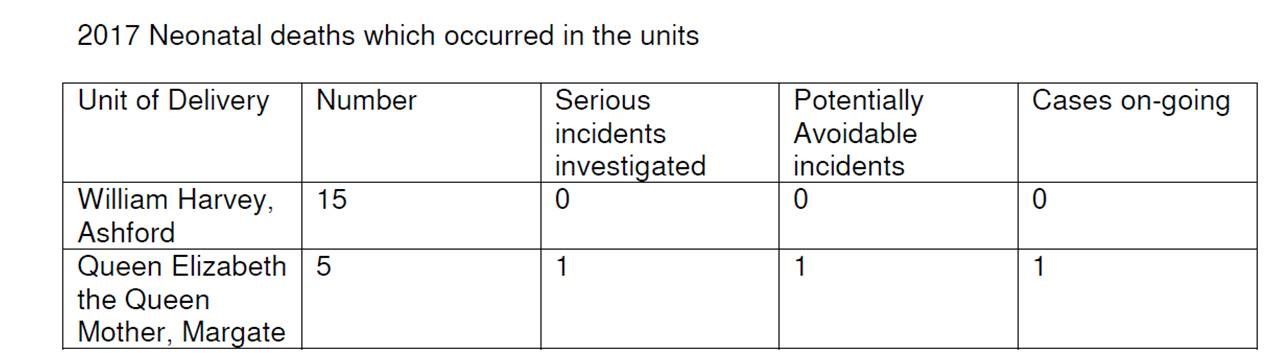
Freedom of Information and Investigations - In FOI 143-19 the Trust show still births and neonatal deaths from 2017 and 2018 and how many deaths were investigated. Link to the FoI is HERE - Looking at Harry's year, 2017 for neonatal deaths we find -
Neonatal Deaths 2017
Unit DeliveredNumberSerious Incidents InvestigatedPotentially Avoidable IncidentsCases On-goingWilliam Harvey15000QEQM5111
The QEQM entry can only be Harry. Therefore, in Harry's year , he was the only neonatal death that was investigated and the only one considered potentially avoidable. However, in the Trust's own board report of April 2017 under "Serious Incidents" is states "Neonatal death due to CTG misinterpretation". Are we really to believe that this death was not investigated and was not potentially avoidable??
All of the following incidents were reported in the Trust's own board reports in 2017 as "serious incidents" it seems beyond astonishing that only Harry's death was investigated and considered avoidable during 2017.
- January 2017 – Maternity incident Intrauterine Death - March 2017 – Maternity Incident regarding a Still Birth
- April 2107 – CTG misinterpretation baby later died - September 2017 – Neonatal overdose of Paracetamol
- October 2017 – A neonatal death - November 2017 - Maternity incident affecting the baby only (Harry)
Reporting to NHSR - Harry's death had to be reported to NHS Resolution within 30 days of the incident in order to be compliant with the Trusts NHS contract. The purpose of this is to ensure that any baby death or one that sustains brain damage is given swift support and the Trust are supported with investigations. In cases of brain damage where the baby survives and where the Trust is culpable, early funds can be arranged for the family too. This tries to ensure early involvement in settlement and reduce solicitors’ costs too. Harry's case was not reported until March 20th, a week after the RCA meeting we had with the Trust which, for them, went very badly wrong. It was reported 108 days past the 30-day deadline. https://resolution.nhs.uk/services/claims-management/clinical-schemes/clinical-negligence-scheme-for-trusts/early-notification-scheme/ Why would this be?
During 2017 the Trust claimed 10/10 for maternity services based on 10 key self-audited very detailed criteria including the one above regarding reporting to NHSR, they received a rebate of well over £1 million for this claim. In 2018 they did the same but following investigation the claims were found to be untrue and they were eventually rejected by NHSR and funds had to be repaid.
Details of the false claims are in the pictures below and can be verified here -
https://resolution.nhs.uk/wp-content/uploads/2020/11/MIS-recheck-database-at-06112020-FINAL.xlsx
In the year 1 claim, 2017/2018 the Trust were asked by NHSR to re-check and verify the claim which they said they did and all was well. It wasn't until much later that they were found, in both years to have failed in 4 out of 10 requirements putting them in the bottom 6% of all Trusts in this maternity safety return.
After the Trusts year-2 claim of 10/10, NHSR audited the results in December 2019 and found that the Trust were only in fact achieving 6/10 and in the bottom 6% of Trusts and the Trust were told to repay the awarded funds. As a result, NHSR audited the year 1 claim that we had initially complained about; they found that the Trust were also in fact at 6/10 and not the 10/10 as claimed. NHSR required the Trust to repay the funds paid. Over two years this was around £2.5 million pounds.
Sir Roger Gale MP challenged Susan Acott the Trust CEO on the year 1 claim and in her response to him on June 7th 2019 said -
".....the evidence we have met the requirements was presented to our full Trust Board on two occasions and also our Quality and Safety Committee. Helpfully our new Chairman is a Professor of Obstetrics and Gynaecology, so we have absolute expertise on our Board. The evidence was peer reviewed with a Trust in West Kent, although this was not a requirement, as well as our commissioners. I have written to NHSR confirming the level of evidence and scrutiny that accompanied the Board sign-off."
6 Months later the Trust were having to repay circa £2.5 million to the NHS following two years of "mis-declared" claims. Snap shot in pictures below, full details here - https://resolution.nhs.uk/wp-content/uploads/2021/03/MIS-recheck-database-Jan-2021.xlsx
Previous History - This Trust had a lot of previous history of issues in maternity, this demonstrated by CCG reports in 2014 and the RCOG report from 2015 as well as CQC inspection reports; additionally, we were able to collate information from board reports that showed they continued to have issues as shown here. When we asked the CEO about the detail in the board reports, this detail stopped being published in their reports preferring to only show a number of serious incidents rather than the detail. So, despite the Trust reporting numerous serious incidents in maternity Harry's RCA was not carried out in the required detail, did not discover the root cause at all. Outside scrutiny from the coroner, CQC and CDOP was actively avoided.
We can all accept that mistakes happen but any right-minded person looking at the evidence above would surely have to conclude that there was either a severe level of senior level incompetence at every possible stage or there was an orchestrated attempt to avoid external scrutiny, and, in so doing, has avoided valuable learning from Harry's death and, we suspect many previous cases let alone the huge delays and increased suffering endured by our family as a result.
Below shows various snapshots. The first two are NHE England's reports showing the Trust falsified claims that they were 10/10 for maternity safety during Harry's time. They later had to return over £1 million to NHSE for the false claims. Below that, showing the severe lack of investigation, the only one, Harry. If you click the newspaper page, it will take you to the Daily Mail story at that time.